There are many respiratory pathologies that limit the ability of horses to perform physical work and therefore affect their sporting performance, and which affect what is known as the «lower airways», which are basically those to which we veterinarians do not have access from the outside.
To give us a better idea of what we are talking about, in this image we can see the different structures that make up the respiratory system of horses:
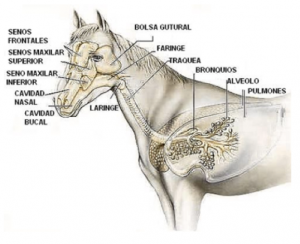
The upper airways are the oral cavity, nasal cavity, maxillary and frontal sinuses, guttural pouch, pharynx and larynx. The lower airways are the trachea, bronchi, alveoli and lungs.
The most common symptoms of lower airway respiratory problems are:
- Cough
- Bilateral mucous or even purulent discharge.
- Epistaxis (nosebleeds).
- Fever
- Dyspnoea (shortness of breath).
- Occasionally cyanosis (bluish mucous membranes due to lack of peripheral oxygenation).
Bronchoalveolar lavage is a procedure used to diagnose respiratory diseases affecting the lower respiratory tract. The purpose of this technique is to obtain a sample of surfactant fluid from the lungs. Our objective is to extract this sample for cytological study and thus be able to check the cellular population, inflammatory component, if there is the presence of bacteria, etc.
How do we perform a bronchoalveolar lavage?
We sedate the patient. The aim is to relax the muscles and reduce the risks of the procedure.
We temper the sterile saline solution so as not to cause bronchospasm when introducing it through the tube.
Wash the nostrils thoroughly to remove any dirt that could contaminate the sample (similar to a surgical wash).
We introduce a special probe through the horse’s nose, which has a balloon in the most distal portion, and a nozzle that fits a syringe in the closest portion.
The probe also has to be perfectly lubricated so as not to cause damage as it passes through all the structures.
More or less halfway, and always with the aim of minimising risks, we inject a dose of local anaesthetic through the probe to numb the whole area and avoid discomfort for the patient.
When we have reached the final area, we fill the balloon with air using a syringe, thus fixing the probe.
We introduce the sterile, tempered saline solution through the tube and wait a few seconds.
We aspirate the tempered liquid and observe how, when we take it out again, a kind of layer with a foamy substance remains, which is the surfactant liquid of the lung. This will contain the cells we are interested in analysing.
We prepare the sample for laboratory study.
Although, as we indicated, the main study is through the microscope, there are other issues that we can observe macroscopically:
- Colour.
- Turbidity.
- Presence of mucus or flocculent substances.
- Odour.
Once analysed in the laboratory, we can obtain a diagnosis of the pathology that is causing our patient’s symptoms. Only with a basic aetiological diagnosis will we be able to prescribe a specific treatment for our patient’s pathology.
